

Before we get into down side of elevated oxalates it is important to repeat something I said my previous post titled Oxalates and MTHFR: Understanding the Gut-Kidney Axis – that oxalates in mild amounts are not a problem for the body. As long as the body can safely detoxify each molecule of oxalate, they will not bother us. Even though they are nasty in high amounts, the body has the ability to get rid of oxalates. We have already seen how proper digestion and gallbladder function protects us from absorbing oxalates. What we haven’t talked about yet is how our body gets rid of oxalates once they enter and build up to toxic levels. Unfortunately life is all about tradeoffs and that principal holds true when it comes to how the body detoxifies oxalates.
Any discussion of oxalates is incomplete without mentioning sulfate. Sulfate is one of the most amazing molecules in our bodies. Sulfate is an essential byproduct of our methylation cycle and without it we cannot survive. Sulfate helps us seal our leaky gut and strengthen our body’s bones, ligaments and tendons; and it is required for Phase II detoxification of all kinds of nasty toxins, hormones and heavy metals. In fact, sulfate is so important for our health that it is the 4th most common nutrient in our blood stream!17
A big reason that oxalates are so toxic is that each oxalate molecule that gets into our body will cause us to lose a molecule of sulfate. The reason we lose sulfate is that oxalate and sulfate use the same transporter to get into our bodies. On the surface of our gut, liver and kidney exists a cellular transporter called the Sat1 transport protein.18 The job of this little cellular micro-machine is to exchange, or swap, one molecule of oxalate for one molecule of sulfate. It is just like a revolving door that constantly pushes sulfate out in exchange for an oxalate molecule coming in. This Sat1 transporter is the reason why we lose sulfate into the gut and into the urine when our oxalate levels rise.19 Consider the following:
Imagine what happens when, as we already discussed, our gall bladder and digestion stops working well. A lot of oxalates from our diet make their way far down into the intestines to the colon. Here the oxalate is floating around and it bumps into the gut wall. On the wall of our colon lives the Sat1 transporter. And what does it do? Well, it will grab onto that oxalate drag it inside our bodies while at the same time pumping out a sulfate molecule. Because we didn’t digest our food well we just lost a molecule we needed (sulfate) and gained one that causes problems (oxalates). If this happens once no big deal; but you and I both know this would happen millions of times at the molecular level. I am confident the body has a genius reason for this, I just haven’t figured this one out yet!
So if our oxalate absorption increases we begin to lose sulfate and this carries serious consequences to our methylation cycle. The loss of sulfate into the gut and into the urine will mean the methylation cycle has to work harder to produce more sulfate, drawing down our nutritional savings account in an attempt to replace what is being lost. For our cells this will cause more resources to be shifted towards detoxification and protection and fewer resources will be invested into growth and repair. Our cells will be stuck in fight or flight and won’t be able to rest or digest very well – and neither will we!
Loss of sulfate can be challenging for the average person and it can be an absolute disaster for someone with MTHFR, GST, GSS, GSR, SULT1A1, 1A2, etc. polymorphisms. These individuals already have a slowed sulfate detoxification system and any loss of sulfate can be devastating to their ability to build, repair and detoxify. Because of the action of the Sat1 transporter when oxalate levels go up, sulfate levels go down.
If losing sulfate wasn’t bad enough, high oxalates also cause our body to lose Vitamin B6. I don’t need to remind you how important B-vitamins are for our health – how they activate our genetic pathways, produce energy, enhance detoxification and allow our cells to survive. Vitamin B6, aka pyridoxine, is a particularly important B vitamin. It has many roles in the body, esp. in the liver where it helps to transform amino acids to promote growth, repair and detoxification. Fortunately this isn’t a biochemistry textbook and I won’t bore you with all the intricate details of how B6 is used in our bodies. What I will highlight for you though is how B6 is very useful in helping people with high oxalates, aka hyperoxaluria.
In a 2011 study looking at individuals with a genetic type of high oxalates, called primary hyperoxaluria type 1, researchers discovered that about 30% of individuals with this genetic disease saw a reversal of their condition when supplemented with Vitamin B6.19 That surprising result is confirmed by another study which was published more than 20 years prior. In this earlier study researchers concluded that giving Vitamin B6 in a high, therapeutic dosage of 5mg/kg/day was effective at reducing the high level of urinary oxalates.20 The patients taking elevated doses of B6 (up to 400 mg per day in some individuals) for 18 months reported no side effects from the B vitamin therapy (how many pharmaceutical drugs can say that?). These studies lend credence to the idea of how safe and effective vitamin B6 can be in people with oxalate toxicity.
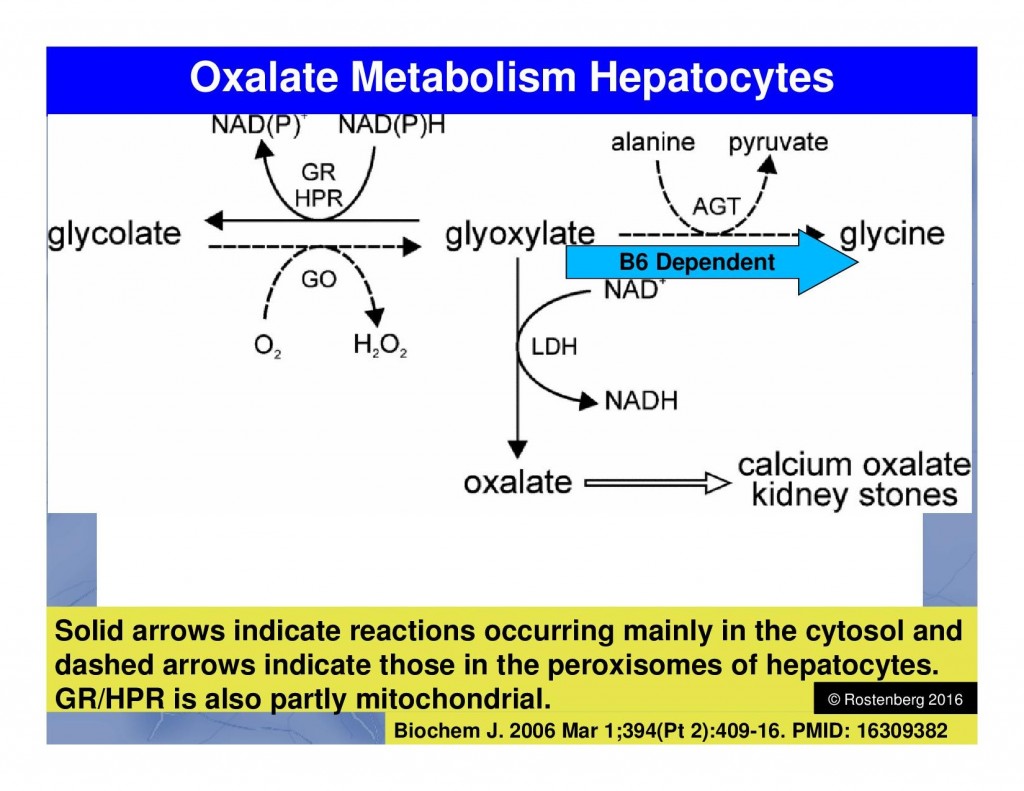 Figure 4.2 – Pathway for oxalate removal and detoxification
Figure 4.2 – Pathway for oxalate removal and detoxification
At first glance it might seem that 5mg per kg per day of a vitamin like B6 is too high of a dose, but there is sound physiologic science behind this idea. The liver enzyme AGT is responsible for converting glyoxylate, the precursor molecule to oxalates, into the much-needed amino acid glycine. 21 Thus the faster the AGT enzyme is functioning, the more rapidly our liver can convert glyoxylate into glycine, preventing the production of oxalates. And since AGT requires B6 to function, we can see how therapeutic B6 levels may be needed to increase the speed and function of AGT leading to fewer oxalate molecules being formed. Genius! Whenever there are elevated levels of oxalates due to a genetic, digestive or metabolic problem, B6 should be considered a useful and effective means to help detoxify this toxin from the body.
The Low Sulfate, High Oxalate Phenotype
Now that we have seen how oxalates can impact our B6 levels, we need to turn our attention again back to the all-important sulfate molecule. By taking a closer look at the oxalate-sulfate connection we will be able to identify the widespread methylation and biochemical problems which are caused by high oxalates. By finding the relationships between oxalates, sulfates, kidney health, hormones, liver detoxification and more we will begin to recognize the high oxalate, low sulfate phenotype.
The big idea with oxalate toxicity is it causes problems in the liver and kidney – our two most important organs of detoxification. While high oxalates will cause liver problems and a loss of B6, it is in the kidney where the oxalate causes us to lose much of our precious sulfate. The kidney is a critical player with any sulfate problem because it is the organ responsible for keeping our sulfate levels in balance.22 The kidney must swap a molecule of oxalate for a molecule of sulfate through the Sat1 transporter, and when oxalates are high it causes a loss of sulfate into the urine. Urine sulfate levels have been a confusing subject for many patients, researchers and doctors who study methylation and genetic pathways. Everyone wants to know where this sulfate is coming from, and I believe the answer has to do with oxalates and kidney polymorphisms.
Many people have used urine sulfate test strips and found high sulfate levels > 1200-1600. This has caused a lot of confusion since very few people know why this happens. There are message boards and chat rooms online filled with pages of perplexing urine sulfate information. Some people say it’s bad to have high urine sulfates, some say it’s good because it means the body is getting enough and spilling the extra. The advice ranges from practical to the absurd, with many deciding to avoid sulfur because of a high urine sulfate reading. But since sulfur and sulfate are essential for our health and wellbeing, I am not convinced that avoiding sulfur based on a urine sulfate test is valid – in fact it’s probably the worst thing you can do!
Remember from the previous post that the most common reason for high oxalates is some kind of chronic gallbladder and gut problem. But not everyone has an oxalate, gallbladder or gut issue, yet they are still dumping high amounts of sulfate in the urine. In these cases the loss of sulfur must be coming from some other problem – and a genetic issue would make the most sense. Similar to our methylation cycle where the MTHFR gene SNPs slow down the activation of folate, there is now research that shows people with certain genes are prone to wasting their sulfate into the urine.
Cutting-edge research has identified that some people have a polymorphism in the NaS1 transporter found in the kidney – the main enzyme for balancing our sulfate levels. While the science is still a bit murky on this, studies have identified two polymorphisms in the kidney that predisposes us to losing sulfate. The NaS1 transporter SNPs were shown to reduce sulfate transport by an incredible 60%-100%.23 This means that for individuals with these NaS1 polymorphisms a massive amount of sulfur is being lost in the urine on a daily basis. If someone with a NaS1 +/+ polymorphism also develops an oxalate problem, then look out because we can expect them to have dangerously low sulfate levels. And you are about to learn how low sulfate levels make us really, really sick!
Could this NaS1 SNP be a major reason why many people are seeing a drastic loss of sulfate into their urine? I certainly think so! And if these individuals with NaS1 polymorphisms see high sulfate in their urine, and then decide to go “low sulfur” can you imagine the problems that will cause? I hesitate to think of it.
Current biochemical research has been providing us with powerful studies that show us what can happen to our bodies when oxalates rise and sulfate levels plummet. To figure out what happens when sulfate is lost in the urine, researchers developed a mouse model that was born without the NaS1 transporter. Researchers basically created a mouse that mimics people who are born with the NaS1 polymorphisms. That is, these mice were born without the ability to absorb sulfate in the kidney and they developed severe sulfate deficiencies! Many of the health problems these low-sulfate mice developed will sound familiar:
Biochemical Problems Associated with the Low Sulfate, High Oxalate Phenotype
- Stunted growth
- Slow metabolism
- Altered behavior
- Decreased insulin function
- Elevated LDL and total cholesterol
- Increased liver stress and fatty liver deposits
- Impaired detoxification and upregulated SULT genes
- Low cortisol, DHEA and adrenal hormone deficiency
- Increased colitis and inflammatory bowel disease
- Decreased mucous production in the gut
- Increased gut permeability (leaky gut)
- Susceptibility to aggressive gut bacteria
- Reduced metallothionein expression and heavy metal detoxification
- Increased size and vascularity of tumors
- Excess serotonin in the blood and decreased serotonin in the brain
- Autism linked to sulfate wasting
Low Sulfate Liver Problems
As many of you know the liver is our main organ for detoxification. This genius organ performs thousands of tasks every second we are alive. We often take what the liver does for granted because it is so efficient at keeping our body in balance. But if high oxalates or genetic SNPs cause us to lose sulfate in the urine then the liver will take a big hit. To understand just how serious low sulfate can be for the liver, we turn our attention to a recent study which looked at what happens to mice when they are born without the NaS1 transporter. In other words, the researchers bred mice that suffered from chronic urine sulfate loss and then they looked at how sulfate loss impacted their growth, detoxification and methylation-related pathways. The results are quite alarming.
To see the effects of low sulfate on the liver we turn our attention to a mouse study published back in 2006. Researchers demonstrated that mice lacking the NaS1 transporter suffered from decreased growth, decreased serum insulin-like growth factor I (IGF-I) levels, altered serum bile acid concentrations, elevated LDL and total cholesterol, fatty liver, upregulation of SULT genes, and hepatomegaly.24 In addition to those major liver stressors, these mice also showed a 71% decrease in metallothionein expression. What this means is that we don’t just lose liver function with low sulfate; we also lose a key part of our methylation cycle. Without metallothionein the body cannot defend itself against toxic heavy metals and is susceptible to neurotoxicity and brain inflammation.25,26 And as we all know, people with chronic disease need all the help with detoxification and inflammation they can get.
Sulfate Loss and Hormones
When sulfate levels are low, the body won’t just have distrubed liver function, it will also suffer with all kinds of hormone problems. The reason why is that the body uses sulfate molecules to inactivate hormones. In a 2008 study also using NaS1 deficient mice, researchers showed that blood levels were reduced 50% for cortisol, 30% for DHEA, and 40% for DHEA-S.27 This massive loss of blood hormones was accompanied by a 1500% increase of cortisol spilt into the urine and lost as well. I don’t have to remind you that losing all this cortisol from the blood and the urine will greatly stress the body’s nutritional and adrenal reserves. It takes a lot of energy and nutritional resources to build a hormone from scratch. And anyone who has suffered with adrenal fatigue can tell you that when the body is tired and run down, it doesn’t do a very good job of building hormones. We know that hormone production requires energy, vitamins, minerals and essential fatty acids – things people with chronic health issues have in short supply.
Consider how the body’s hormonal needs are always changing. We need different hormones at night than during the day, different hormones during rest and play, and women who are menstruating need different levels of hormones throughout the month. Suffice it to say our hormonal needs are always fluctating through our days, months and years of life. Luckily the body has developed a genius method for balancing our hormone levels – it sulfates them. Rather than spending energy removing a hormone only to have to build another one to replace it, the body inactivates steroid hormones by attaching a sulfate molecule.
In fact, many of the hormones we test for in clinical practice such as progesterone, estrogen, cortisol, and DHEA are stored in the blood in a sulfated form. And clinicians often order tests for DHEA-S, Progesteron-S, etc. to look at the blood levels of the sulfated hormones, helping to give a more detailed picture of the hormone levels in the body. The body uses sulfate molecules to keep the hormones in circulation, to store them until later when the body needs to reactivate them. In this way the body is more efficient because it can activate and inactivate a hormone by simply removing a molecule of sulfate. This takes much less effort than building a hormone from scratch every time! So when sulfate levels are low or non-existent, there is a severe drop in hormones.
Low Sulfate and Gut Problems
Seeing how we’ve already gone in-depth looking at how high oxalates and low sulfate disrupt health, I wish we could end our discussion here. But if I did I wouldn’t give you the whole story, including how loss of sulfate drastically impacts our gut health. Now that we have seen how low sulfate creates liver and hormone problems, we must turn our attention to another critical part of our health. As we’ve covered several times already, gut health is the foundation for the health of every other system in our body. And the balance of our gut microbes determines in large part the health of our gut. We simply cannot have a healthy digestive system if we cannot sustain and maintain healthy bacteria in our colon and small intestine.
Just like bugs and insects in the forest need a place to live and food to eat, so too do the gut bugs in our bowels. To provide our gut bacteria with a sustainable living condition, the cells which line our gut produce mucous. This mucous coats and protects our own cells while also providing food and shelter for the bacteria we depend on for survival. And since we cannot make mucous without sulfate, any low sulfate problem will create a gut issue.
Current research highlights just how big of a problem low sulfate is for our digestive system. In a study published in 2009 researchers discovered that low sulfate mice suffered with inflammatory bowel disease, decreased mucous production, leaky gut and aggressive bacterial infections.28 A more recent study published in 2014 confirms that low sulfate, in addition to slowing growth and liver function, has a major negative impact on gut function.29
The important take away here is that once the body loses sulfate, mucous production in the gut is interrupted. Since our good, healthy probiotics depend on the mucous for survival, any loss of mucous production will lead to a loss of healthy probiotics. Without a healthy mucous layer, the cells which line our gut will be unable to defend themselves against toxins, while aggressive bacteria will injure and inflame the lining of our gut. Keep in mind that sulfate is required to build strong molecular bonds, like the bonds in our skin, cartilage, bones, and other connective tissues. It is also required to make mucous be sticky and coat the lining of the bowel. If the body is depleted of sulfate, either because of a kidney polymorphism or an oxalate toxicity, then mucous production and gut health is going to suffer.
Low Sulfate Cancer and Autism
We have just about covered the gamut discussing oxalates and sulfates, but there are still a couple items left to address before we close. I have two more pieces to this oxalate-sulfate puzzle that must be shared. As if it weren’t enough that low sulfate seriously hampers our liver, hormones and gut function, studies also show that low sulfate impacts serotonin levels, cancer growth and autism spectrum disorders. We all know that cancer, depression and developmental disorders like autism spectrum disorders are now epidemic in our society, but few people realize how low sulfate can make these problems worse.
To understand how low sulfate impacts cancer, researchers looked again at the NaS1 -/- “low sulfate” mouse model. The researchers studied how very low sulfate levels can alter tumor growth; and the results they discovered are astounding! In a study published in 2010 researchers discovered that tumors grew 12 times faster and had more than double the blood vessels in the low sulfate mice vs the normal sulfate mice.30 When mice have cancer and low sulfate at the same time, the cancer thrives in that environment and becomes much more aggressive. This suggests a critical role for sulfate to play in keeping our body healthy, and lacking sulfate makes it that much more difficult to overcome a chronic disease like cancer. Now we aren’t as simple a creature as a mouse, but we share a lot of the same biochemistry. Isn’t it possible that people will also suffer more aggressive cancer if our sulfate levels drop? The evidence suggests this is a real possibility.
When researchers turned their attention to low sulfate and serotonin, they found that neurotransmitters are also greatly impacted by sulfate issues. Researchers in 2007 used low sulfate mice and found that blood serotonin levels doubled while brain serotonin levels were reduced by about 12% compared to normal mice.31 At first a study like this doesn’t sound very important, but lets breakdown what these scientists are saying. They are pointing out that when sulfate is lost in the urine (as happens with high oxalates) then serotonin cannot be inactivated and turned into serotonin-O-sulfate. The body cannot control the levels of neurotransmitters because it lacks the ability to turn them off!
Can you imagine how challenging it would be for our body to live without sulfate and the ability to inactivate our hormones and neurotransmitters? What a mess! Since these mice lacked the ability to “turn off” their serotonin they ended up with way too much of it floating around. And it might seem like a good thing to have higher serotonin; and that thought also crossed my mind. But when we look at the bigger picture and realize that our body also uses sulfate to “turn off” many other hormones, we can see a potential disaster here. Without sulfate in our bodies we not only lose control of neurotransmitters, we also cannot balance our other critical hormones that keep us healthy. And given how many people are suffering with adrenal fatigue, infertility, menopause, andropause and other hormone issues, it’s obvious that low sulfate is a much bigger problem than most of us think!
The research on sulfate is amazing partly because of how many different conditions are related to it. And this is especially true of the Autism epidemic, where sulfate is critical for children with ASD concerns. Remember that in order for our body’s detoxification system to work correctly we need sulfate molecules available (technically we need the PAPS molecule, a close derivative of sulfate). Our liver takes sulfate molecules, which are produced by the transulfuration part of the methylation cycle, and glues them to stuff we need to get rid of. The body glues sulfate to drugs, hormones, toxins, heavy metals and other garbage that we must eliminate in order to be healthy. And you don’t have to be a doctor or a researcher to know that children with Autism have a problem with detoxification and thus they have a problem with sulfate. Anything that lowers the availability of sulfate for their body to use is going to be a problem for autistic children. And that is precisely why high oxalates and low sulfate levels are especially harmful for these kids.
While the cause of autism remains uncertain, we do know that the issue is getting much worse. If it seems like more and more children are being diagnosed with autism, then you are right. The latest data from the CDC shows that rates of Autism continue to skyrocket. Rates of autism were only 1:150 in 2000 but are now impacting 1:68 in the year 2010, with boys affected 5 times more often than girls at a rate of 1:48.32 If the CDC’s own data wasn’t enough of a shocker, we have some cutting-edge PhD research that paints an even darker picture.
Autism rates are growing so fast that according to Dr. Stephanie Seneff, PhD, a research scientist at MIT, we can expect to see 50% of all children with autism by 2025. This number might sound preposterous, but Dr. Seneff is a mathematics expert and bases her calculations on the current rate of increase. In other words if we don’t change the rate at which ASD issues are occurring, her numbers will come true in 10 years!
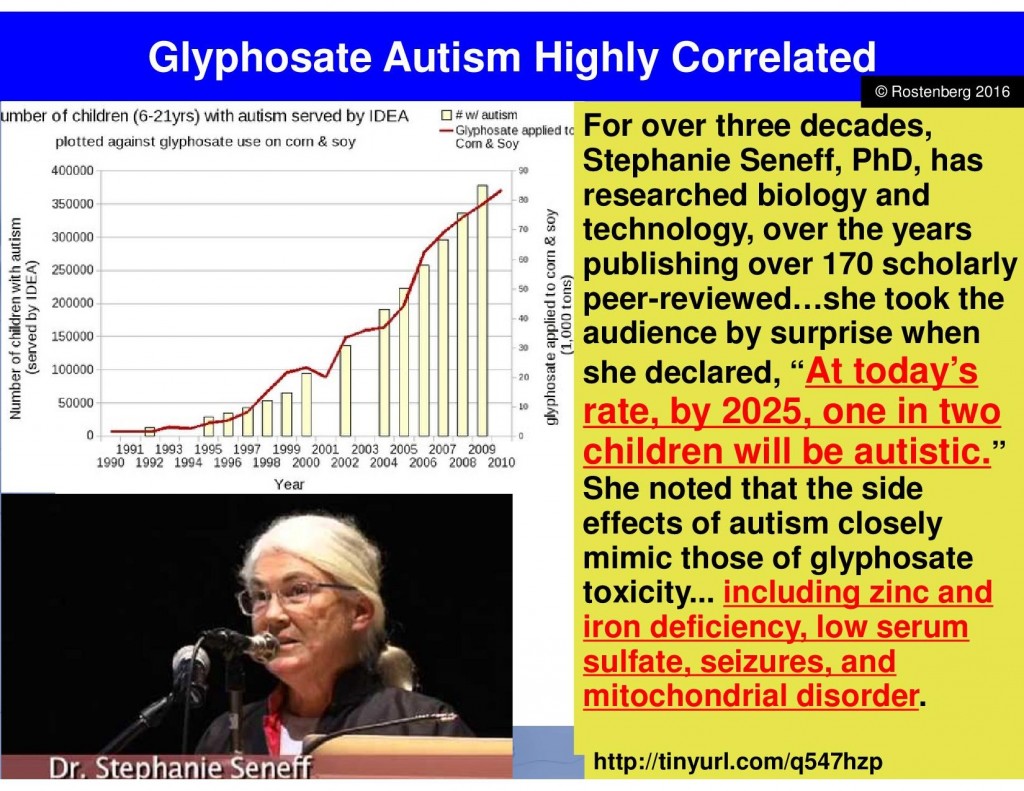
Figure 4.3 – 2013 research study showing correlation between use of glyphosate and rise in Autism Spectrum Disorders in the United States.
Another important aspect of Dr. Seneff’s research relates to the increasing ASD rates and the use of genetically modified food sprayed with the toxin glyphosate. She has highlighted the connection between genetically modified foods and the poisons used to grow them compared to the rates of ASD.33 I will admit that correlation is not causation, so more studies are needed to confirm this. But at the same time there is a clear relationship between use of glyphosate and increasing rates of autism disorders. I would not recommend eating GMO foods while we wait years for more studies to prove the toxicity of these genetically modified “foods”!
In one final study to share with you on oxalates, researchers wanted to see if there was a connection between autistic individuals and urine sulfate levels. In a study published in 2013 researchers investigated austitic children to determine if they had NaS1 SNPs and measure how much sulfate they lost in the urine. They found 78% of autistic children have NaS1 kidney polymorphisms and that 60% of these autistic children with this polymorphism end up wasting high amounts of sulfate into the urine.34 This confirms that austistic children are prone to low sulfate levels. This study doesn’t carry a ton of weight by itself, yet when we consider the impact that low sulfate can have on our bodies it begins to make a bigger impact.
We’ve discussed above how low sulfate leads to changes in growth, behavior, gut function, immune health, and slower detoxification. Clearly these health issues are well known problems for individuals struggling with ASD. I want to clarify that I am not saying that low sulfate is the cause of autism. However given how sulfate is important for the health of our cells, it’s obvious that anything which lowers sulfate levels will put stress on our bodies. Since those with autism already face many hurdles, any additional biochemical stress on these patients should be avoided at all costs. This is why it is so important to look at oxalate and sulfate issues with all patients who are dealing with chronic health concerns like ASD and developmental issues.
Conclusion
As we close this chapter I want to reiterate that oxalates are an important part of the chronic disease puzzle. Due to the fact that oxalates injure the kidney and reduce the function of the liver, we need to be aware of oxalates in our diets and bodies. This is especially true in individuals who are living with serious methylation problems! People who don’t methylate well already have a susceptibility to stress, toxins and gut problems. Adding an oxalate problem on top of that just creates another often unrecognized hurdle for the body to overcome.
Despite the potential toxicity of oxalates and the fact they can be found in much of our food, our body is well equipped to deal with this food-born toxin. The mechanism our body uses to prevent oxalate problems is very simple – it just requires that our gallbladder and gut is healthy! This is why we always, always make sure the gut is functioning as we begin to help patients heal. But since gut health is usually ignored and not understood in our health care system, we will likely see more oxalate issues creating chronic health problems. In my practice we address oxalate problems right away, and you can too, by following the advice in the Protocols section or contacting my office directly.
For more videos and learning about Oxalates, Gut and Methylation I recommend:
Organic Acid Test – An Essential Tool for Gut-Methylation Problems
Oxalates and MTHFR: Understanding the Gut-Kidney Axis
In Health,
Dr. Rostenberg
By studying the current peer-reviewed research, Dr. Rostenberg has discovered powerful, natural strategies to optimize gut and methylation function to heal the body. He can help you uncover the genetic or root causes of your health problem and find a natural solution! If you would like help balancing your oxalate levels to improve your methylation cycle and reduce/eliminate your symptoms, please contact Dr. Rostenberg at Red Mountain Natural Medicine today. Phone 208-322-7755. Email redmountainclinic@gmail.com. Website http://www.redmountainclinic.com
For more recipes, dietary guides and general information on oxalate issues please visit Susan Owen’s websites:
Low Oxalate Info website & Trying Low Oxalates facebook page
REFERENCES
- Ostojic, SM eds. Steroids – From Physiology to Clinical Medicine. 1st ed. InTech, November 21, 2012 under CC BY 3.0 license. Accessed on June 12, 2015.
- SLC26A1 – Sulfate anion transporter 1. Uniprot.org web site. www.uniprot.org/uniprot/Q9H2B4. Accessed on October 27, 2015.
- Robijn S, Hoppe B, Vervaet BA, et al. Hyperoxaluria: a gut-kidney axis? Kidney Int. 2011 Dec;80(11):1146-58.
- Mitwalli A, Ayiomamitis A, Grass L, et al. Control of hyperoxaluria with large doses of pyridoxine in patients with kidney stones. Int Urol Nephrol. 1988;20(4):353-9.
- Behnam JT, Williams EL, Brink S, et al. Reconstruction of human hepatocyte glyoxylate metabolic pathways in stably transformed Chinese-hamster ovary cells. Biochem J. 2006 Mar 1;394(Pt 2):409-16.
- Markovich D. Physiological roles of renal anion transporters NaS1 and Sat1. Am J Physiol Renal Physiol. 2011 Jun;300(6):F1267-70.
- Lee S, Dawson PA, Hewavitharana AK, et al. Disruption of NaS1 sulfate transport function in mice leads to enhanced acetaminophen-induced hepatotoxicity. Hepatology. 2006 Jun;43(6):1241-7.
- Dawson PA, Gardiner B, Grimmond S, et al. Transcriptional profile reveals altered hepatic lipid and cholesterol metabolism in hyposulfatemic NaS1 null mice. Physiol Genomics. 2006 Jul 12;26(2):116-24.
- Stankovic RK, Chung RS, Penkowa M. Metallothioneins I and II: neuroprotective significance during CNS pathology. Int J Biochem Cell Biol. 2007;39(3):484-9.
- Yu X, Guo J, Fang H, et al. Basal metallothionein-I/II protects against NMDA-mediated oxidative injury in cortical neuron/astrocyte cultures. Toxicology. 2011 Mar 28;282(1-2):16-22.
- Dawson PA, Gardiner B, Lee S, et al. Kidney transcriptome reveals altered steroid homeostasis in NaS1 sulfate transporter null mice. J Steroid Biochem Mol Biol. 2008 Nov;112(1-3):55-62.
- Dawson PA, Huxley S, Gardiner B, et al. Reduced mucin sulfonation and impaired intestinal barrier function in the hyposulfataemic NaS1 null mouse. Gut. 2009 Jul;58(7):910-9.
- Markovich D. Na+-sulfate cotransporter SLC13A1. Pflugers Arch. 2014 Jan;466(1):131-7.
- Dawson PA, Choyce A, Chuang C, et al. Enhanced tumor growth in the NaS1 sulfate transporter null mouse. Cancer Sci. 2010 Feb;101(2):369-73.
- Lee S, Kesby JP, Muslim MD, et al. Hyperserotonaemia and reduced brain serotonin levels in NaS1 sulphate transporter null mice. Neuroreport. 2007 Dec 3;18(18):1981-5.
- Baio, J. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2010. Surveillance Summaries March 28, 2014 / 63(SS02);1-21.
- Swanson NL, Leu A, Abrahamson J, et. al. Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 2014.
- Bowling FG, Heussler HS, McWhinney A, et al. Plasma and urinary sulfate determination in a cohort with autism. Biochem Genet. 2013 Feb;51(1-2):147-53.




Despite your assertion that B6 is safe and free of side effects, there is an awful lot of sick people who find this B vitamin very hard to tolerate, especially when it triggers neuropathy even at low doses.
Hi Troy,
Its not my assertion that B6 is safe and free of side effects. That is the assertion of the researchers who performed the study on oxalates. I would agree that one person’s solution is another person’s poison. Everyone is unique and there is no one-size-fits-all protocol. Many people tolerate B6 at very high doses. Those who do not tolerate B6 often have a Lysine deficiency and that is the bigger issue.
In Health,
Dr. Rostenberg
I was one who developed neuropathy by taking too much B6, compounded by the doctor assuming I must be low in B6 and giving me more before deciding to run a test, and my level was something like 165 when it should be more like 25 or below. By then I was visiting a neurologist, who decided not to run other tests because he was sure that the B6 was the source of my problem and had me completely avoid any supplement with B6 (not any in real food), and it took over a year for my levels to come down, with the neuropathy decreasing along with it. There was never any mention of lysine, but I find that interesting and wish my doctors had known more. I am learning so much on this site!!!
I am suffering from B6 toxicity. I was taking supplements that contained massive amounts of B6 that I was unaware of. I am also +/_ MTHFR C677T with numerous snps such as +/+COMT V158M, +/+COMT H62H, +/+MTRR A66G, +/+ MTRR A664A, and +/+ VDR Taq, +/- CBS C699T . I also believe that my B6 toxicity started years ago when I was taking smaller amounts found in multivitamins as I’ve had nerve problems for years. It finally became known after taking the much larger amounts more recently. Is the reason I’m B6 toxic because of my impaired methylation?
Hi Christe,
Thanks for your comment. You need Lysine in order to utilize B6 and many, many people are low in lysine. That would be the first place to look. Also taking high amounts of B6 may cause a relative deficiency in other B vitamins.
In Health,
Dr. Rostenberg
This is encouraging news!
I’ve not been able to tolerate B6 for many years and no doubt is contributing to my severe disability. Is there a ratio of lysine to B6 that is important? Or do you recommend taking lysine for a few weeks before trying B6 again?
Also, last question: Can lysine cause an increase in ammonia levels? Conflicting info online…
Thank you in advance.
What are was to boost sulfate?
Hi Deana,
Thank you for your comment. We boost sulfate with epsom salt baths, cruciferous vegetables, supplementation like NAC, glutathione, taurine. Also fixing the oxalate issues, improving digestion, supporting methylation and detoxification, and managing stress effectively (lowering cortisol) is very helpful in increasing sulfate levels.
In Health,
Dr. Rostenberg
This was extremely helpful and informative. I really appreciate learning this information. However, I am more confused about sulphates/sulphur than ever now. I appear to have an oxalate problem but I also appear to have a sulphur problem. According to my CBS snp I am supposed to follow a low sulphur/sulphite diet. So where does that leave me in regards to what is being said here?
Hi Carrie,
Thanks for your comment. Sulfur isn’t a bad thing, in fact its essential. Don’t follow a diet based on genes! Follow a diet based on the needs and requirements of your body, of the environment around your genes. Your best bet is to save time and money and work with a practitioner who is knowledgeable in these facets of our biochemistry. I would love to help you find your path to a better, healthier you. Please call my office 208-322-7755 or email us at redmountainclinic@gmail.com.
In Health,
Dr. Rostenberg
What tests are suggested to determine if one has a sulfate problem? I know I have an oxalate issue.
Hi Brenda,
Thanks for your comment. Once you confirm you have an oxalate issue, then you have also confirmed you have a sulfate problem. They go together!
In Health,
Dr. Rostenberg
Would it be beneficial to take (MSM) sulfur supplements if a person has high oxalate problem?
Hello Fahad,
Thanks for your comment. Yes, MSM is a good source of sulphate for the body. Another source is epsom salts and of course cruciferous veggies are high in sulfate as well.
In Health,
Dr. Rostenberg
I’m with Carrie on the sulfur problem. Your gut protocol is very high in sulfur veggies because it is low oxalate, and being on that protocol and some of the high sulfur supps that go with it made my back spasms worse, maybe because of increased ammonia. When I went off all the sulfur foods except protein, and the sulfur supplements, my spasms were better than they had been in years, but the oxalte issues creeped back (painful shoulders and harms). So I really do need someone who can work with a person who has both oxalate AND ammonia problems. Is that you guys? Are you as experienced in ammonia issues as you are with oxalates? Thanks!
Hi Julie,
Thanks for your comments! Ammonia is produced in every cell in our bodies. We have a mechanism to get rid of it and that is the urea cycle in the liver. If the liver is sluggish and unsupported then the urea cycle can slow down and ammonia levels rise. Also, when the body becomes acidic the urea cycle is slowed down to conserve bicarbonate which helps to alkalize our tissues. When we have anything affecting our liver, if we are acidic or if we are breaking down our muscle tissue (catabolic state) then we produce more ammonia than we can get rid of effectively. Ammonia can be treated effectively with activated charcoal and targeted amino acids like ornithine, citrulline, etc. to address the imbalance in urea cycle. In cases where ammonia is a problem we like to perform the Great Plains urinary amino acids test (spot first thing in the morning works best). This test accurately shows us what is going on in the urea cycle as well as many other pathways of interest. I recently worked with a five year old patient who couldn’t run or speak in sentences because he was suffering from ammonia-induced encephalopathy. He was treated with NADH, ornithine, and other supplements and three months later he was running around and having conversations with his mother. Pretty amazing!
Please contact my office if you would like to schedule a consultation to discuss this in more detail.
In Health,
Dr. Rostenberg
Oops, that was arms, not harms.
And one more question about gluconeogenesis. If Ammonia is naturally produced in the body during “gluconeogenesis”, which is part of the breakdown of fats and proteins to be used for energy, then does that mean a diet higher in fat and protein than carbohydrates will also generate more ammonia than a high carb diet? Thanks!
HI Dr Rosenberg,my Dr. had me taking statin drug called Simvastatin and i told her i wouldnt take it anymore because of the side effects ,that it causes memory loss.So she gave me something else called Welchol and i am not taking because it makes me sick,I have gained weight and i have never weighted more than a 110 lbs, I am not sleeping at all at nite and dont want to take those awful sleeping pills. I have been light headed and dizzy. I would prefer to take natural suplements, Could tell me what supplements to take.. Thanks Jeanne
Hi Jeanne,
Thanks for your comment. Sounds like many patients I talk to that you are not enjoying the “standard” medical approach as the side effects are worse than the problem itself! Well it is safe to say you do not have a drug deficiency. Very likely you are experiencing a form of Adrenal Fatigue that is altering your metabolism, digestion and blood pressure. I suggest you look at my Adrenal Fatigue protocol page. The supplements which will be the most helpful in cases such as this are the following:
For Moderate Stress, including dizzyness, craving salt, and painful joints/muscles –
Licorice Plus – 1-4 per day herbal support that will increase cortisol naturally and improve blood flow; helps prevent dizziness and increases tolerance to stress.
Cortico B5/B6 – Take 1 am w/ food, 1 noon w/ food. High doses of B5 and B6 and Vitamin C necessary to produce Coenzyme A (CoA), a key energy molecule; also helps with adrenal hormones and supports healthy response to stress and low blood sugar.
Biosom – Take 1-6 dosages per day. Dissolve 20 seconds then swallow. Liposomal DHEA which helps combat low sex hormone levels and improve resistance to stress and immune health.
You can find this information on the Adrenal Fatigue page under the Protocols section of BeyondMTHFR.com. Stay strong…you will be better! And as always, if you need more assistance a consultation with myself or one of our highly trained doctors is a great way to get you on your way to better health naturally. Our office may be contacted at 208-322-7755 or redmountainclinic@gmail.com.
Yours in Health,
Dr. Rostenberg
I had my child (who is on the spectrum) on a low sulfur diet. Then I put him on a low/medium oxalate diet. He definitely responded. About a month later I started giving him Epsom salt baths. Clearly, he needed it. That was about a year ago and now I give him taurine daily and Epsom Salt baths weekly. However, recently I tried expanding his diet by including black eyed peas (a sulfur food). He came home that day saying he was sad and crying, which is really out of the norm. I am wondering, should I try to increase sulfur foods again more slowly or just leave things as is? Also, as of note we support his methlynation cycle and add L- Ornithine to help with ammonia issues. In addition to being low oxalate we are low in phenols/ salicylates as well. I know they are connected but I cannot figure out how to get past it. Thanks!
I’m doing better than I have in a long time though so I can’t complain. You are right I did NOT have a drug deficiency! I DO better when taking lysine and B6. I DO better when addressing my liver and gallbladder (soluble fiber to discourage bile re-circulation, good ol beans, thanks Karen Hurd) I DO better when making sure I have sufficient stomach acid. I just have one problem! (Well that is a severe understatement actually) but when I eat sulfur foods and soak in epsom salts, I STINK. It comes out through my skin in the pits of my groin. I can’t stand it. I feel everyone can smell me. It’s in the sweat. Do you recommend sauna sweating to deal with it? Does this mean I am not utilizing any of the sulfur? Is there something I am missing that would make me more able to break it down? Thanks for your article.
Thank you for a really good article. This has really helped to explain how certain symptoms and areas of knowledge I have link together. Has also filled in some missing areas that hopefully will help me to resolve some issues I am dealing with. Many thanks.
Sulfate as well as a-hydroxybytuyrate is very low in urine organic acid test. At the same time unable to tolerate NAC because of confirmed SIBO. In this situation I am thinking Vitamin B-6 is the only solution . Can glucosamine sulfate be of any help?
Many Thanks.
Hi Vivek,
Thanks for your comment. Epsom salt baths are a good way to introduce sulfate to your body without taking oral sulfur supplements or foods. That is a good choice for people with SIBO.
In Health,
Dr. Rostenberg
I have just begun passing a few calcium oxalate kidney stones in the past 12 months and have no family history of stones except my 86 father recently had his gall bladder removed. I am female, hypothyroid, 61 yrs of age, have been vegan for 5 years, walk 6-8 miles per week. I have also been diagnosed with osteoporosis. In my 40’s I was having some pain in my hip and went to a rheumatologist who (with a visual examination of my nails) diagnosed me with psoriatic arthritis. He put me on a treatment plan of doxycycline and diclofenac with quarterly monitoring of my blood. I did this for 4 years until I questioned and ultimately decided to quit this treatment of my own accord. I’ve had no pain since. I honestly think he would have kept me on this protocol forever. Also, during this time I was diagnosed with HPylori and took antibiotics for that as well. I was retested later to confirm the HPylori was gone and it was. My urologist does not seem well versed on prevention of kidney stones but has ordered the 24 hr urine kit for me at my request. I should be getting it soon. I have increased my water consumption to more than 6 12 ounce glasses per day and I’m beginning to lower my oxalate foods. I’m also eating yogurt with calcium along with my meals. I’m finding myself very confused about all the information and misinformation on so many sites I’ve been to, including the foods that are considered low oxalate. What are the main steps I need to do to find out the root cause of my kidney stones so that I can prevent them? Also, is the low oxalate food list you recommend by Susan Owens a list that has been scientifically tested to show true oxalate levels? There is a lot of variation online.
Can one cause a B6 deficiency from taking high doses/long term of lysine? thanks
Hi there,
I would like to know if anyone has any thoughts on how to treat a very bad h.pylori infection without using anything containing high oxalates. I am extremely sensitive to oxalates and intolerant of vitamins and minerals to support my gall bladder and metabolism of them.I have only recently being having major issues with this infection and I actually cannot function without treating it somehow. Problem is supplements like mastic gum is related to the cashew/pistachio family so undoubtedly high oxalate and other supplements and herbs commonly used to inhibit its growth are also far too high, such as oil of oregano, thyme oil, grapefruit seed extract etc Anyone know how I get around this issue or is it even possible? Thank you.
I tried a high dose of p5p (b6) 165 mg in one shot and 10 minutes later had nausea so bad I vomited. So I assume that means I’m probably low in lysine? I have >1600 urine sulfate on test strips and many of the SNPs (waiting on organic urine acid test to come back), wanted to take the high B6 (5mg/kg) to start treating it. So how should I dose the lysine to p5p? 500mg lysine to 165 mg p5p?? Thanks, learning so much from your articles which are explained very well!
Hi Dr. Rostenberg,
your article makes so much sense to me!
I have horrible reactions to oxalates PLUS I have very, very low levels of DHEA-sulfate and Pregnenolone-sulfate!
Would it make sense to test for both hormone forms, Dhea & Dhea-s, pregnenolone & pregnenolone-s to see if only the sulfated form is deficient?
I am already eating a low oxalate diet, so are there other reasons for sulfate-wasting ? Because my hormones are still low.
Thank you for your great research!
Hi Michelle,
Thanks for your comment. You can be sure that if DHEA-S and Pregnenolone-S are low then the non-sulfated forms of the hormones will be low also. Your body uses the sulfate molecule to put excess hormones, which are not needed at the moment, into storage. Essentially the sulfate molecule inactivates the hormone without destroying it, so your body can reactivate it when needed. Adrenal fatigue is another common problem that leads to decreased sex steroid and hormone levels. Many people with oxalate issues also have adrenal fatigue of some sort, so that is often another cause we see in our patients.
In Health,
Dr. Rostenberg
Great article . I have developed salicylate and histamine issues since going grain and dairy free. I’m assuming that substituting potatoes for my carbs increased oxylates . Have you seen people resolve histamine and salicylate issues by going on a LOD? I’m eating a lot of cabbage and doing Epsom salt foot soaks every other day while decreasing my oxylates .
Hi Stacey,
Thanks for your comment. Many people have seen improvements with an LOD as you say, however for long lasting change you need to look at the deeper reasons to why oxalates created a problem in the first place. Salicylates actually break down into oxalates via the glyoxylate pathway (video + article to come), so lowering oxalates helps your body detoxify salicylates. I believe that most if not all salicylate issues are in fact oxalate issues masquerading as something else. If you would like more help individually, please contact our office 208-322-7755 and care@redmountainclinic.com.
In Health,
Dr. Rostenberg
my nutreval shows my lysine levels are very good and my b6 is very low but i have b6 toxicity
hey Dr. Rostenburg would taking Epsom Salt orally increases sulfate levels in the body.
Hi Calvin,
Epsom salts taken orally will give you a large dose of magnesium which will cause a severe laxative effect. It is better to soak feet or take a warm bath with Epsom salts to get the sulfate levels increased inside the body.
In Health,
Dr. Rostenberg
My daughter is 18 and on progesterone only birth control. she has high oxylates in her urine. I am wondering if you know if this birth control is interfering with her digestion or creating this problem?
Hi Linda,
Thanks for your comment. While I don’t know of any direct relationship between progesterone birth control and oxalate issues, there is a possible link. Progesterone, like estrogen, places strain on the gallbladder’s and liver’s detoxification pathways. If the birth control is compromising liver and gallbladder function (as birth control often does) it could then cause a dysfunction in the gut by interfering with bile function. If the bile isn’t working correctly when we eat food, even healthy stuff, we can start to absorb higher amounts of oxalates than we normally would. If that goes on over time then oxalate problems could develop. To look into this deeper you would do well to schedule a consultation with our office. Our team is trained to know how to get to the root cause of these types of issues. You can reach us at 208-322-7755 and care@redmountainclinic.com. Hope that helps!
In Health,
Dr. Rostenberg
Dr. Rostenberg,
Finally!! Someone putting the pieces together to explain why my son’s ulcerative colitis has been refractory to so many of the “best” protocols (including years of Metagenics products – some of which contain folic acid!). Although we’ve known about his homozygous methylation defects for almost 2 years and epigenetics is in its infancy, I believe this knowledge will change the approach of allopathic medicine … it has to. I imagine you get a lot of flack from that side of the fence.
Your blog explains his tendency to form kidney stones (3) and he’s 23, his potential C-diff, and his stubborn ulcerating colon. As we’ve just been told by the head gastroenterologist at Baylor College that “there is not enough well-vetted knowledge about ulcerative colitis and the methylation system for anyone to be able to make reliable recommendations in that respect” and “a colectomy may give the best quality of life outcome.” I whole-heartedly disagree.
Thank you for actively engaging with people asking questions in your blog and for your efforts to educate. We are in the process of reaching out to your office but don’t know if remote help would be sufficient in our case.